Our favoured disc
Currently our usual recommendation is for the M6-C disc as it has been designed to replicate the normal motion and mechanical behaviour of a human disc as closely as possible. It is “an almost true physiological copy of a young disc” and achieves this though a cunning design strucutre.
M6C and M6L Artificial Cervical and Lumbar Disc
- Replicates the anatomic structure and biomechanical performance
- Controls range of motion in all 6 degrees of freedom
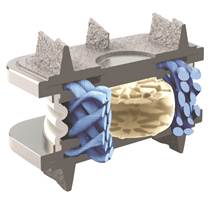
- Compressible viscoelastic polymer nucleus simulates native nucleus
- Surrounding multi-layer high tensile strength WPE annulus
- Simulates progressive resistance to motion of capsule
- Physiologically almost an exact match for a young disc
- More robustness
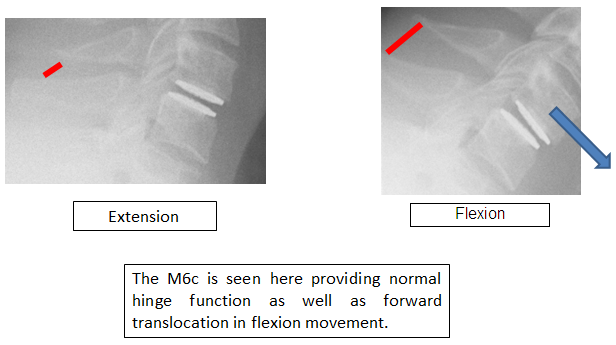
The M6 artificial discs have a nucleus and an annulus, that replicate the normal function of the nucleus pulposus and annulus fibrosus. They allow both compression and translation whilst controlling and progressively limiting movement in all directions.
For up to date information regrarding M6 artificial discs, please press here.
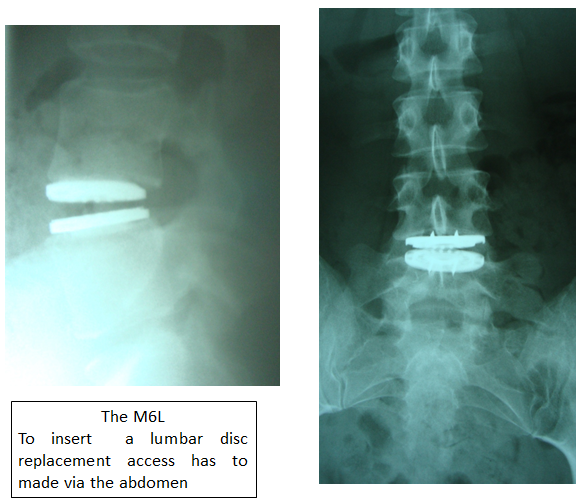
There is an artificial disc for the cervical and the lumbar spine – The M6C and M6 L
The design of the M6 discs allow for the restoration of full movement. The sizes available are design to completely cover the end plates of the vertebrae so as to prevent the bones fusing around the disc
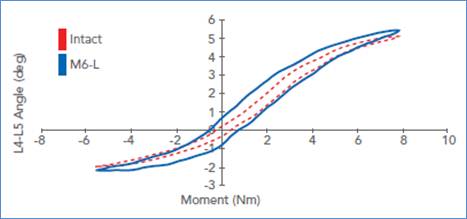
This graph shows the resistance to movement throughout the normal range of an intact healthy disc vs the M6C. Not quite perfect but the other designs offer virtuall no resistance at any point and do not change at all as the movement builds.
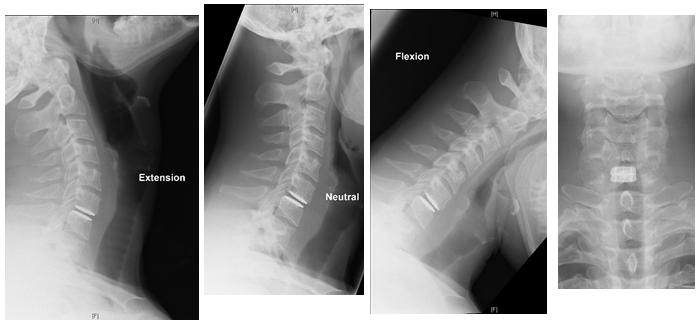
Like all all artificial discs currently available the M6c has a metal end plates made of titanium. This is a hypoallergenic metal which is MRI scan compatible ie you can safely have MRI scans afterwards should you need them. The M6c infact causes virtually no disturbance of the images so clear pictures of the operated level can be obtained following surgery.
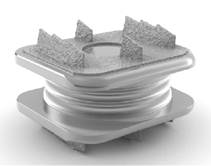
The surface of these metal endplates have micro-pores like a spongy surface into which the bone of the vertebrae grows. After some months the bond is very strong. Even heavy contact sport like rugby can usually be resumed at six months post surgery – should you wish and, in our opinion, providing you have been given the correct one!.The plates often have fins, as in the M6c, which help secure the device in the early days and enhance this bond.

The vertebra facing surface of a disc replacemnt is designed with micropores into which the bone grows so as to fix the device in place.
The fins seen here on the M6L assist in early fixation and strengthen the bond between the bone and disc replacement
How long will my disc last?
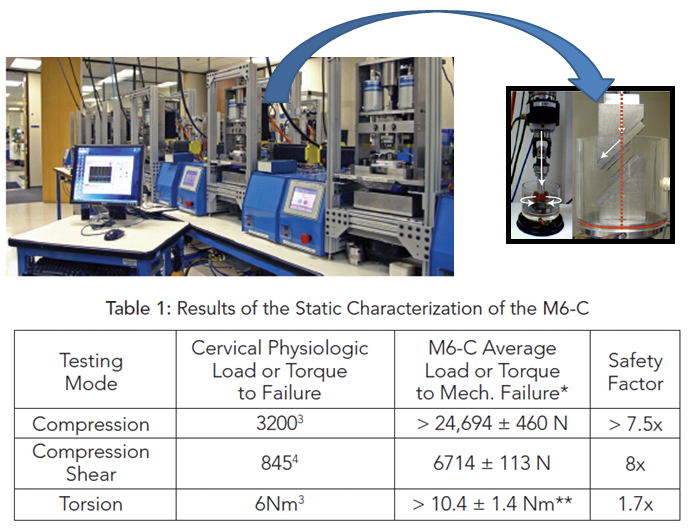
The truthful answer is that we do not know. We have patchy long term follow-up on some of the older designs. These designs have been improved on and so inevitably the newer devices have not been used for the many decades that it needed to see if they actually live up to our expectations. They are tested in laboratories on rigs that simulate strains hugely in excess of that of normal life and for considerably longer than a normal life time. There are large margins of safety built in. However, a normal disc must have some capacity to heal which an inert implant has not. Our experience of all implants is that they wear out and may need replacing. The options then are to convert to a fusion or exchange the old disc for a new one. Disc replacements have been around for many years and we have yet to see large swathes of folk coming back with worn out prosthetics. Your great grandchildren may be able to tell you more certainly than us. What would we do? I think we have already answered that!
Which disc should I have?
There are few good comparative trials and even the simple long term follow up studies are flawed. In addition their results drive change and the newer discs are always only supported by shorter term data. Countries vary as to which discs are available. The process of getting a disc to market is much slower, and some might say safer, in the USA than for example Europe. Indeed the people of the USA where the M6 disc was developed have been coming to Europe to get it! We have given you our current view. Other reputable groups are using some of the alternatives. Certainly in years to come we will all probably be making different recommendations. The Spine Surgery London will continue to independently assess which one or ones in our opinion offer the better current option. Our surgeons have used all the ones you have seen and some others besides. We do not own shares in any of them and perhaps you can see why! Be you a patient or a manufacturer we are always open to your suggestions as we are to the proponents of fusion over disc replacement. If you think we have missed anything out which is material to this debate please tell us as we want to know and would like to tell our patients.